THE SANITATION PARK
PROJECT
Rhonda Bower, Leonie Crennan & Arieta Navatoga
SOPAC Secretariat
February 2005
SOPAC Technical Report 386

THE SANITATION PARK PROJECT
A REGIONAL INITIATIVE TO INCREASE PARTICIPATORY APPROACHES IN THE SANITATION SECTOR
Prepared by
Rhonda Bower, Leonie Crennan & Arieta Navatoga
SOPAC Secretariat
February 2005
SOPAC Technical Report 386
This Project was funded by the New Zealand Agency for International Development and the World Health Organisation
[2]
Cataloguing in Publication Data:
Bower, Rhonda (et al)
The Sanitation Park Project : A regional initiative to increase participatory approaches in the sanitation
sector/Rhonda Bower. Ł Suva : SOPAC, 2005.
21 p.: ill.; 30 cm
ISSN:
1605-4377
1. Sanitation engineering 2. Sanitation engineering Ł Fiji Islands
I. Crennan, Leonie
II. Navatoga, Arieta
III. SOPAC Technical Report 386 IV. Title
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[3]
TABLE OF CONTENTS
ACKNOWLEDGEMENTS .................................................................................................................................................4
1
PROJECT EXECUTIVE SUMMARY .......................................................................................................................5
2 BACKGROUND .......................................................................................................................................................6
Overall
Objective .....................................................................................................................................................6
Purpose
...................................................................................................................................................................6
Outputs
....................................................................................................................................................................6
Target
Group ...........................................................................................................................................................6
Project
Duration .......................................................................................................................................................6
3 PROJECT
ACTIVITIES ...........................................................................................................................................7
Pre-project surveys .................................................................................................................................................7
Phase 1 ...................................................................................................................................................................8
Park Construction of the demonstration wastewater treatment systems (March Ł November 2003)..............8
Sanitation Park Signage .................................................................................................................................8
The Community Programme of the Sanitation Park Project .....................................................................................8
Hands-on composting toilet construction training, Suva, 7-11 June 2004 .....................................................10
Community Workshops WHO/MoH "Healthy Islands Initiative" in Keiyasi, Balevuto and Nadelei .................12
Keiyasi
Workshop
15th Ł 17th June 2004 ...............................................................................................13
Balevuto Workshop 21st Ł 22nd June 2004 ............................................................................................16
Nadelei
Workshop
1st Ł 2nd July 2004 .................................................................................................17
Sanitation Park Opening Ceremony, 18 November 2004.......................................................................................19
4
PROJECT CONCLUSIONS AND RECOMMENDATIONS ....................................................................................20
Recommendations from Construction of Sanitation Park ......................................................................................20
Recommendations from the Community Programme ............................................................................................20
Conclusions
...........................................................................................................................................................21
ANNEXES
A
Pre-Project Survey Information April 1st Ł 30th April 2000 ..............................................................................22
B
Hands on Training Workshop Participants List, May 2004 ............................................................................32
C Community Healthy Islands Workshops Participants Lists, June 2004..........................................................33
D Keiyasi
Action Plan ........................................................................................................................................36
E Balevuto
Action Plan......................................................................................................................................38
F Nadelei
Action Plan........................................................................................................................................39
G MOU
Project Partners....................................................................................................................................41
H List
of
Acronyms ............................................................................................................................................47
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[4]
ACKNOWLEDGEMENTS
We acknowledge the World Health Organisation (WHO) and the New Zealand Agency for
International Development (NZAID) through their New Zealand Pacific Initiative for the
Environment (NZ-PIE) scheme for the financial assistance provided to the Project.
Appreciation goes to the tireless efforts of the Project Team over the four years of the Project and
we gratefully acknowledge their special skills, knowledge and support given right up to the
successful conclusion of the Project.
A big vinaka vakalevu to:
Ę The Fiji Ministry of Health (MoH), the national agency responsible for design, implementation
and monitoring of rural water supply and sanitation projects and programmes in Fiji. MoH
played a significant role in the Project, linking it with the communities in Fiji through their
network in the various districts.
Ę The World Health Organisation (WHO), the UN agency responsible for environmental and
human health, and poverty alleviation through improved water supplies, sanitation and
hygiene. In addition to providing funding, WHO was also a key partner in providing technical
support from the Project start.
Ę The Fiji School of Medicine (FSchM), the regional organisation responsible for the training of
Environmental Health Officers for the health ministries of Pacific islands governments. We
would like to thank FSshM for accepting the Sanitation Park to be part of their School Campus
linking it with the students and its associated training programmes.
Other partners to whom we would like to pay tribute include:
Ę Rakesh Dayal and his team for the excellent work in constructing the systems at the Park and
also assisting in facilitating training when called upon;
Ę John Robinson for the artwork provided for the signs; and
Ę Graphic Systems for professionalism in delivery of the signage, a sample is pictured on the
title page of this report.
We sincerely thank the communities of Keiyasi, Balevuto and Nadelei for welcoming us into their
villages and homes and for their role and cooperation in the Project.
Though the Project Team was inclusive of officials and representatives of the World Health
Organisation, Fiji Ministry of Health, the Fiji School of Medicine; and SOPAC, the officials making
up the core Sanitation Project Team were:
Dr Keshwa Nand
Ł Fiji School of Medicine
Mr Navi Litidamu
Ł Fiji School of Medicine
Mrs Vasemaca Naulumatua Ł Ministry of Health
Mr Timoci Young
Ł Ministry of Health
Dr Leonie Crennan
Ł SOPAC
Ms Rhonda Bower
Ł SOPAC
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[5]
1: PROJECT EXECUTIVE SUMMARY
A genuinely grassroots undertaking with full community involvement, the Sanitation Park Project
is designed to provide support to communities in Fiji in identifying and solving their sanitation
problems by examining and selecting from a range of appropriate, affordable wastewater
treatment options housed at a demonstration park located at the Fiji School of Medicine,
Tamavua Campus.
The Project Team including the World Health Organization (WHO), Fiji Ministry of Health (MoH),
Fiji School of Medicine (FSchM) and the South Pacific Applied Geoscience Commission (SOPAC)
worked together to implement the Project with funding provided by WHO and the New Zealand
Agency for International Development (NZAID).
Three rural communities namely Keiyasi (Sigatoka), Balevuto (Ba) and Nadelei (Tavua) were
selected as suitable locations for Project implementation through pre-project surveys. This
included hands-on training for the construction of a composting toilet in May 2004 involving
district health workers and community members; and three community Workshops under the
WHO "Healthy Islands Initiative". The Workshops in the three communities assisted them to
develop action plans using the Healthy Islands process, which will be managed by the local
health officers in the future.
The Project, although implemented in Fiji, has regional application through adopting technologies
that are applicable to other countries within the Pacific and the location of the Sanitation Park at a
regional training institute Ł the Fiji School of Medicine. FSchM will use the Sanitation Park as a
training tool and the information will be available to regional students undergoing health services
training there.
FSchM will manage the Sanitation Park and use it in appropriate training programmes both for its
students and for other members of communities, schools and other teaching institutions and
leaders. The Sanitation Park can also be used for awareness raising and training purposes by
other groups promoting appropriate technology in sanitation.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[6]
2: BACKGROUND
Government bodies and the public have tended to give little attention to sanitation issues in the
Pacific. This complacency and subsequent lack of investment has led to inadequate development
in the sanitation sector. The result is an absence of good training facilities for Health Workers and
Technicians, with health education in the community suffering in particular. Ultimately, there have
been serious health consequences for the community. The lack of awareness of the importance
of appropriate excreta disposal leads to little or poor maintenance of existing sanitation facilities,
resulting in low standard waste disposal systems.
As a result of the above, sanitation related diseases are prevalent in the community,
predominantly in rural areas and squatter settlements, where poverty is rife. Ultimately the marine
environment, water resources and sub-soil suffer due to dangerously high levels of faecal
contamination.
Overall Objective
Reduced number of sanitation related diseases, reduction in the pollution of the marine
environment, water resources and sub-soil in the Pacific.
Purpose
To assist communities in the implementation of appropriate excreta disposal technologies whilst
developing the skills of health workers, sanitation technicians and students of Environmental
Health.
Outputs
Sanitation Park containing various demonstration wastewater treatment systems located
at the Fiji School of Medicine, Tamavua Campus.
Hands-on composting toilet construction training in May 2004 involving district health
workers and community members from three selected communities namely Keiyasi
(Sigatoka), Balevuto (Ba) and Nadelei (Tavua).
Community Workshops in June 2004 under WHO/MoH "Healthy Islands Initiative" in
Keiyasi (Sigatoka), Balevuto (Ba) and Nadelei (Tavua).
Multiplier effect with replication in other Pacific island countries (through the regional
students at FSchM).
Target Group
Beneficiaries of the Project included the communities of Keiyasi (Sigatoka), Balevuto (Ba) and
Nadelei (Tavua), District Health workers in the three selected communities and FSchM students
from various faculties.
Fiji was specifically the focus of this Project because it is the only island (apart from Papua New
Guinea) that has the facilities to train sanitary engineers. There is also a distinct lack of
community-based sanitation work going on in Fiji.
Project Duration
April 2000 Ł December 2004
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[7]
3: PROJECT ACTIVITIES
The Project was implemented by the Project Team in two distinct components: (1) the Sanitation
Park containing various demonstration models of wastewater treatment systems with the
associated signage; and (2) the Community Programme, which included the hands-on
composting toilet construction training and community workshops under WHO's "Healthy Islands
Initiative" banner.
Prior to the Project implementation however, pre-project surveys were carried out in early April
2000 to identify communities in which the Community Programme component would be carried
out.
The various activities carried out during the course of the Project are elaborated on below:
Pre-Project Surveys
A quantitative justification was required for Project implementation in the chosen communities, as
there was an unclear picture of community status with regards to sanitation in Fiji during the initial
stages of the Project. The quantitative justification was obtained by carrying out surveys for more
detailed and accurate data from the communities throughout Viti Levu, Fiji, from 1 to 30 April
2000.
The pre-project surveys were carried out in order to determine the extent of sanitation-related
problems in the various communities. At this stage, the Project Team relied on the local
knowledge of its partners (Fiji Ministry of Health and the Fiji School of Medicine) to identify
communities in Fiji that were known to have sanitation problems. Potential locations were
considered in the rural interior, rural coastal, and squatter settlements of Viti Levu.
District Health offices in Ovalau, Kadavu and the Western and Central divisions of Viti Levu, were
contacted by the Ministry of Health in early 2000 and asked to identify communities that are
experiencing sanitation problems. A checklist was sent out to district offices with set questions
regarding the present sanitation situation in the communities. Each office was given two weeks to
complete the checklist and identify three `problem' communities consisting of a rural interior, rural
coastal and a settlement community. The exercise resulted in the identification of 14 communities
on Viti Levu in which the surveys were carried out.
The objectives of the pre-project surveys being to:
identify the sanitation problems that exist within the problem communities;
determine the level of priority that the communities attribute to their sanitation problems; and
determine the extent of sanitation-related disease in the problem communities via recall as
well as clinic data.
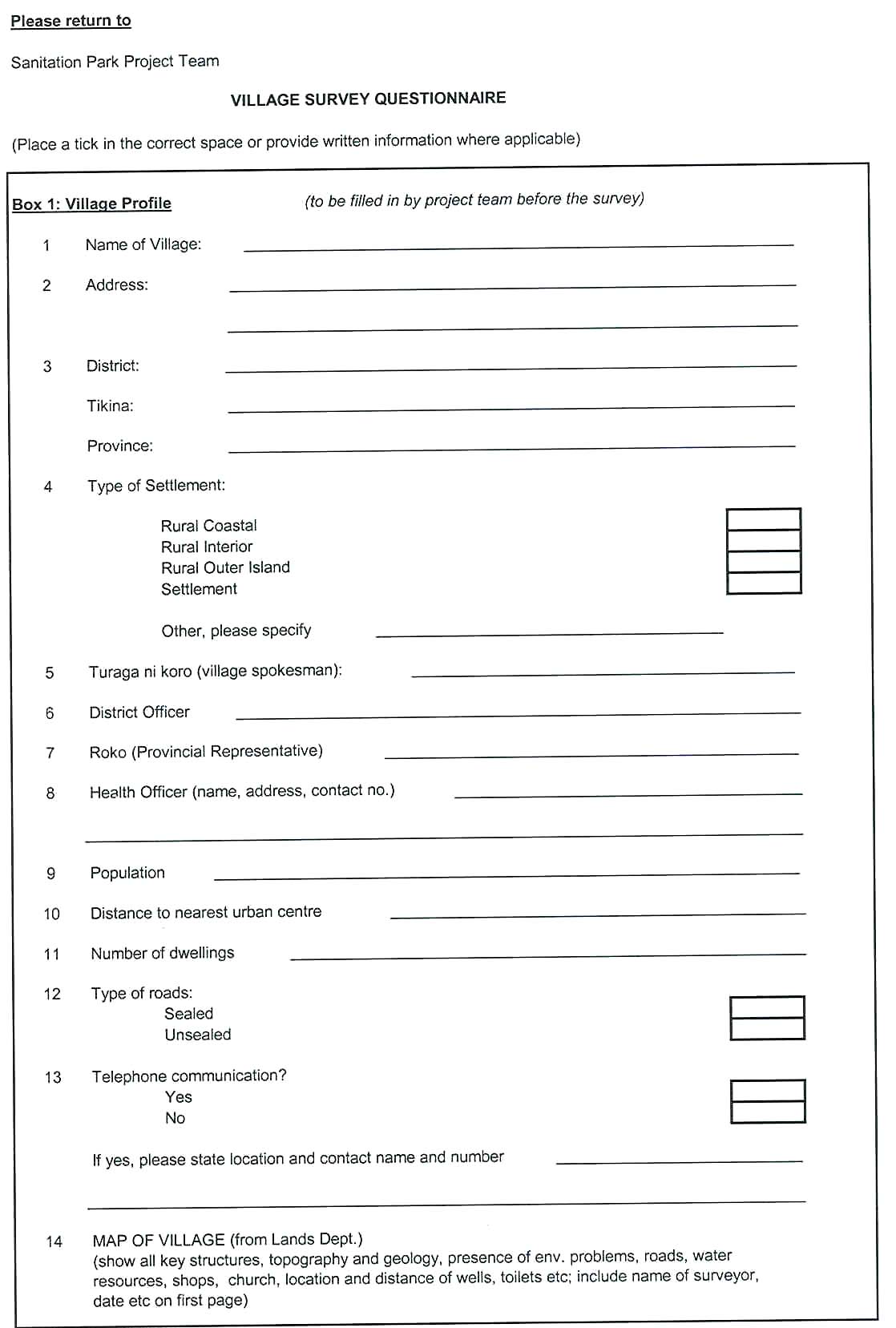
The surveys consisted of three components: household questionnaires; GIS data gathering; and
water quality testing. Results from the survey in fourteen communities around Viti Levu, Fiji were
analysed to assist with identifying three communities to be targeted for Phase 1 of Project
implementation (see Annex A for Pre-Project Survey Results).
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[8]
On review of the results, three villages were recommended as the most appropriate for actioning
Phase 1 of the Project, these being Balevuto in Ba; Keiyasi in Sigatoka; and Nadelei in Tavua.
Important criteria in taking this decision included communities identifying sanitation as a priority
for community development.
Phase 1
Phase 1 of the Sanitation Park Project involved the Project Team carrying out the most
substantial part of the Project, which included the following:
Sanitation Park Construction of the demonstration wastewater treatment systems (March 2003 Ł
November 2003)
The "Sanitation Park" is a demonstration of a range of systems, beginning with low technology
facilities to progressively higher-level treatment systems, in a "sanitation ladder" of available
treatment and disposal options. The "Park" provides an opportunity for interested community
members, students, leaders and community health workers to examine how the wastewater
treatment options work to treat excreta and protect human health.
The Project Team had initially considered employing a construction company to design and
construct the Park but it was decided it would be a more effective learning experience for all
concerned if the Project Team undertook design and installation themselves.
Project Team members contributed to the designs for various systems and discussed the layout
for the Park. A local builder was hired to undertake the construction. The site provided by FSchM
was challenging as it was in a small steep gully at the back of a public clinic. Initially it was
decided by the Project Team to locate the sanitation systems around the edge of the gully, in a
manner, which would simulate a village setting and allow access to the systems for inspection.
The systems would then be connected with a path to allow users' comfort and easy access when
viewing the systems. The layout was later modified because of the difficulty and cost of
construction in the gully in the very wet conditions that occurred in Suva in March and April 2004.
Consequently the systems were all built close together on one side of the gully.
Unfortunately the ventilated pit latrine VIP was built next to the sanitary well. This was corrected
with signage and fencing. It was initially planned that the well be sited next to the CT, as it is one
of the advantages of the CT that it can be close to water sources without causing contamination.
The septic tank was also sited close to the VIP and was separated through a partition.
Appropriate signage has been developed for each system making it clearer.
The systems at the Park have been developed to provide an interactive learning environment
featuring cut-away and viewing portals in the various systems to provide maximum
communication between viewers and the system. Viewers will also comprehend actual sizes of
the systems and get a feel for material used. Additionally the systems will serve as a technical
training tool for use by FSchM in their teaching programme with their students.
Sanitation Park Signage
The signage created for the different systems were primarily developed based on ideas of
the Project Team with some input from participants of the Hands-on Training at FSchM in
May 2004.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[9]
Several considerations taken into account when developing the signs are outlined below:
Ę Language, agreed signs would be in English to accommodate the fact of limited space
on signs. Any translation would be taken on board by FSchM in their future training
programmes, on material to be developed by them to complement the systems;
Ę Information on materials, costs, operation and maintenance should also be included in
signs. Again due to limited space this could not be accommodated but can be taken up
in the future by FSchM for any further material development;
Ę Cross-section diagramme of system, showed various parts and how they worked;
Ę All signs were standardised in design, color, font and style; and
Ę Signs accommodated features to combat weathering and vandalism as much as
possible.
After the concept was developed, much consultation was carried out by the Project Team to
agree on final signage information and presentation. This was then taken to a professional
sign making company (Graphic Systems) to transform the ideas and concepts to actual
signage output. This whole process took around six months. The Project Team also
solicited the support of a free-lance artist John Robinson to provide necessary artwork for
some of the signs.
The final product for signage was computer generated and printed on PVC and installed at
the park site with supervision by the Project Team in November 2004.
The Community Programme of the Sanitation Park Project
The goals of the Community Programme of the Sanitation Park Project were to provide
accessible information on the comparative value of a range of common sanitation systems,
including design, appropriate location, preferred and alternative materials, cost to build,
maintenance requirements, health benefits and risks. It was intended that community participation
in this programme occurs in three stages:
Ę Hands-on Composting Toilet Construction Training in May 2004 involving district health
workers and community members from three selected communities namely Keiyasi
(Sigatoka), Balevuto (Ba) and Nadelei (Tavua). This experiential training allowed
participants, including district health workers and community members, to construct a
composting toilet with a view to participants returning to their villages and work places with
these skills and knowledge and sharing these experiences with their respective
communities (see Annex B: Hands on Training Workshop Participants List, May 2004).
Ę Community Workshops held, June 2004, under WHO/MoH "Healthy Islands Initiative" in
Keiyasi (Sigatoka), Balevuto (Ba) and Nadelei (Tavua). The workshops facilitated by the
Project Team in the communities, built upon the hands-on-training held in May 2004,
supported the Sanitation Park construction. The main purpose for the community
workshops was to mobilize the village participants to develop action plans under the
"Healthy Islands" approach and used this as an opportunity to highlight wastewater issues
(see Annex C: Community Workshops Participants Lists, June 2004).
Ę Ongoing inspections and demonstrations at Sanitation Park for the public and
environmental health students.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[10]
Hands-on Composting Toilet Construction Training, Suva, 7-11 June 2004
The Hands-on Composting Toilet Construction Training commenced on 7 June 2004 with the
arrival of the course participants in Suva. The Project Team met with the participants to welcome
them, to provide them with protective clothing such as overalls, gumboots and hard hats for
construction work, and explain the course programme.
The participants included a community representative elected from each of the villages of Keiyasi,
Balevuto and Nadelei and a District Health Officer from each of their districts.
On 8 June 2004 the participants assembled at FSchM, Tamavua Campus, and an introduction
was provided by Project Team members Mr Navi Litidamu, Senior Lecturer/Assistant Head of
School Administration, School of Public Health & Primary Care at FSchM and Mr Timothy Young,
Senior Health Inspector, from the Ministry of Health (MoH). A number of students from FSchM
joined the training and over the three days the number of participants fluctuated between 12 and
25. Two Peace Corps Volunteers participated as observers. A senior member of Vunisinu Village
(Rewa), Mr Pita Vatucawaqa, accompanied one of the Peace Corps Volunteers as they planned
to install and trial a `Wheelibatch' composting toilet in his village as part of the International
Waters Project.
The participants were shown around the Sanitation Park site where the following demonstration
systems had been constructed over the preceding eight weeks:
Ę sanitary well;
Ę a ventilated improved pit latrine (VIP);
Ę a septic tank and soakage trench with viewing portal; and
Ę the foundations and partially-completed concrete block work chambers of an alternating
batch composting toilet (CT) or organic toilet.
The goal of the hands-on training was to provide the technical skills to build a composting toilet in
their village, or to build the systems for others as an income-generating activity if desirable. The
training focussed on completing the composting toilet, as this was an unfamiliar sanitation system
in Fiji.
The participants from the three villages were informed that, in the second component of the
community programme for the Sanitation Park Project, when the Project Team visited their
villages as part of the Workshops under the Healthy Islands Initiative, they would be required to
present what they had learnt during the construction training. This would also serve to reflect what
they had understood from the training and what they had considered to be useful and important.
Despite constant rain and muddy conditions at the site, the participants constructed the following
CT components over two days:
Ę drainage system from plenum floor of the composting chamber to a blockwork trench
which was lined with plastic sheeting and filled with aggregate and stones;
Ę treated pine slat false floor in composting chamber;
Ę access door to the composting chamber, with baffles to allow inspection without contact
with the composting pile; and
Ę toilet room floor with toilet pedestal and ventilation.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]

[11]
Figure 1:
Community representatives,
FSchM students and Health
workers during the hands-on
composting toilet training at
FSchM, Tamavua Campus, Suva.
The builder, Mr Rakesh Dayal, took an active role in allocating tasks and demonstrating
construction. He then supervised while the participants built the components of the system. Mr
Dayal is a competent builder and encouraged the participants to produce quality work. He had not
acted in this teaching capacity previously but demonstrated patience and skill in this role. The
Consultant, Leonie Crennan, supervised the overall design and instruction process but few
interventions were necessary as the participants worked enthusiastically under Mr Dayal's
direction and asked many questions.
In the group there was one female Environmental Health Officer and four female trainee health
officers. As the men were inclined to step forward first to undertake the carpentry and masonry
work, the women were given the task of constructing the drainage trench for the second
composting chamber. In addition to this specific designated task, they observed the building
process and asked questions with the other participants.
A fibreglass toilet seat or pedestal had been purchased by SOPAC from the Development Officer
at the Central Planning Department in Tonga to use on the demonstration model. However the
design needs to be modified and a mould made for production of pedestals for general use in Fiji.
On the third day, an indoor session reiterated the principles of construction and maintenance of
the ventilated pit latrine, the septic tank, the sanitary well and the CT.
To reinforce understanding and management of the CT, the design of two different types of CT's
were discussed, and a short video was shown of alternating batch toilets being maintained in rural
and urban settings in Australia. This was followed by a DVD entitled `Water Tomorrow', produced
by the Asian Development Bank, with assistance from SOPAC, which examined efforts in Tonga
and Kiribati to deal with contamination of ground water from domestic rubbish and human
excreta. A variety of approaches, which involved communities in more responsible and informed
environmental management were demonstrated. In the discussion following these presentations,
the participants covered the following issues:
Ę It was useful to know that environmental health officers and community members were
tackling the same problems in Tonga, Kiribati and Fiji, and that various methods of
community participation and education were being tried.
Ę Seeing families using the CT in Australia demonstrated that there is also a need for this
kind of toilet in developed countries, and the system can be modified for use in a modern
urban house or a rural setting.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[12]
Ę The main obstacle to implementation of the CT in the villages would be maintenance such
as collecting and using the leaves to be added as a carbon/nitrogen mix, and emptying the
compost at the end of the decomposition process.
Ę The CT would be very helpful in villages where there was a water supply problem.
Ę How could the CT seat be cleaned as water should not be put down the toilet, and would
there be a problem with drainage if people who used it had diarrhoea?
Ę What would happen with the CT in a flood?
Following the session on management of the CT, details on construction and maintenance of the
VIP, the septic tank and trench, and the sanitary well were presented by Mr Keshwa Nand, a
Project Team member and Lecturer School of Public Health & Primary Care at FSchM.
In addition to the hands-on training, a field trip was also organised to a settlement in Suva called
Makoi to inspect an alternating batch CT built by Greenpeace in 1996. The system used fishing
net instead of a timber false floor to support the compost pile with the net being removed when
the compost is ready to be emptied. There had been reports that the CT was not popular with the
local residents and it was intended to ask them what their experience of the system had been.
However there were not any residents available for discussion at the time of the visit. It appears
that the fact that the CT was a communal unit was a disincentive for maintenance. This is a
common experience with CTs in other locations in the Pacific and it is recommended that a CT be
used in an individual domestic context unless it can be guaranteed that it will be maintained by
designated person/persons.
The group also visited the Vector Control Centre where concrete toilet pedestals for pour flush
and pit latrines are cast.
After the field trip the group returned to FSchM to discuss the presentations that they would be
making to their community as part of the workshops planned in each of their villages over the
following weeks.
The participants reported that it had been very useful to be involved in a practical interactive
training course where they had learnt new technical skills. The next step would be conveying this
information to community members back in the village. The participants requested that the media
shown to the group as part of the workshops be brought to the village so they could use it in their
presentations.
Community Workshops held in June 2004 under WHO/MoH "Healthy Islands Initiative" in Keiyasi
(Sigatoka), Balevuto (Ba) and Nadelei (Tavua)
During the preceding months the two-day village workshops had been planned through co-
ordination with the District Health Officers in the MoH. The MoH planned to conduct the `Health
Promoting Communities (HPC) Workshop' in the village, as part of the Healthy Islands (HI)
programme, and `Sanitation Park' would be a component of their environmental health discussion
and promotion. A collaborative effort with these fieldworkers, who had developed an ongoing
working relationship with the communities, was seen to be an effective way to introduce
Sanitation Park and associated personnel to the community, and also to integrate sanitation into
the environmental health of the village as a whole.
The aim of the Healthy Islands Programme is:
Ę to develop an understanding of the design and principles of the Health Promoting
Communities programme;
Ę to familiarise village participants to the five steps and six action areas in the healthy islands
approach;
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]





















[13]
Ę to establish a Health Promoting Community or village;
Ę to identify factors which influence health-promoting practice in the villages; and
Ę to recognise the contribution of villagers and stakeholders in health promotion.
It was planned that, on the second day of the two-day Workshop, each village would prepare an
action plan based on the discussions on the first day.
It was agreed that the SOPAC and FSchM Team members take a supportive role in logistics,
provision of multi-media and technical advice if required, while the local officers would facilitate
the workshops in co-operation with community leaders and participants.
Keiyasi Workshop 15-17 June 2004
Figure 2:
Keiyasi women
involved in discussion
and planning during
their two-day
workshop.
On June 15 the Project Team travelled from Suva to Sigatoka and met with the district
environmental health officers at the Ministry of Health office. The Project Team then travelled to
the village of Keiyasi deep in the Sigatoka Valley and met with the Village Spokesman who was
an active participant during the two days of the Workshop.
A Women's Church Group provided meals and the Team was billeted in homes in the village. A
second group of women took care of catering on the second day, which meant that the
responsibility and the funding was shared around. This involvement also ensured that the whole
village was aware of the Workshop.
Representatives from three other villages besides Keiyasi also attended the Workshop. There
were 43 participants from Keiyasi, Navula, Sawene and Edrau. A Peace Corp Volunteer from the
Provincial Office at Korovou attended as an observer (he had also been at the training in Suva for
half a day) and he planned to pass on information about the sanitation systems to other
environmental and coastal protection programmes in the district.
On June 16, the Workshop opened with prayers and a sermon by the local Pastor focusing on the
connection between cleanliness and godliness, followed by an introduction by Mr Timothy Young.
Ms Vasemaca Naulumatua, Project Team member and Health Inspector from Nadi (Ministry of
Health) explained the Healthy Islands Programme. Threats to environmental and public health
were raised such as poor drainage, inadequate disposal of rubbish and the impact of domestic
animals within the village.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[14]
Mr Mesake Biumaiwai, the Headman of Keiyasi, who had been a participant at the training in
Suva, then presented his understanding of the demonstration models at Sanitation Park, and in
particular the construction of the CT using a slide show prepared by the Consultant. The local
District Health Officer, Mr Penioni Cagilaba who was also present at the hands-on training,
assisted him. Discussion and questions followed such as:
Ę Should the dry leaves be kept close by the CT? Yes.
Ę How long does the waste take to decompose? Six to twelve month.
Ę What happens to the compost if you have diarrhoea? The pile will absorb it.
Ę What kind of toilet paper can you put in the toilet? Anything that will decompose.
Ę Can you use detergents to clean the inside of the toilet seat? Just use a rag with a stick and
drop it in the toilet or wipe with vinegar or bicarb of soda.
Ę Is there a plastic container inside the hole? No.
Ę How many years will the toilet system last? The same time as a concrete block house if it is
properly built.
Ę Can ash be used instead of dry leaves? Yes but best to use dry leaves as well.
Ę Why are you promoting the CT and how can this toilet be built in our village (funding,
materials etc?). To provide a choice, and assistance can be requested through the usual
procedure where government/village share cost on a two thirds/one third basis.
It was observed that both women and men were actively involved in the discussion and the
women asked many of the questions.
The DVD, "Water Tomorrow" and video footage of CTs in Australia was also shown at the
Workshop. The village generator was required when this media and Power Point presentations
were being shown.
In the last session of the first day the community representatives were requested to prioritise the
environmental issues in their village, which required attention. This was in preparation for their
Action Plan to be developed the following day. A representative from each village then presented
their priorities to the Workshop. All villages had improved toilets and water supply in their list of
priorities.
On the second day, 17 June 2004, two medical students from FSchM presented a village profile
of Keiyasi, which they had developed from a survey conducted in previous months. The
Sanitation Park Project could be incorporated into this component of the FSchM student
programme by including the student survey of Keiyasi in the Project. This data included number
and type of toilets in a percentage of houses, drainage problems, and certain diseases detected
in the surveyed group, such as diabetes, skin disorders, elevated blood pressure and obesity. For
the rest of the day, the community representatives developed their Action Plan, which included
time frame and persons responsible to undertake remedial, or development initiatives. A
representative from each village then presented their action plans to the other Workshop
participants (see Annex D for Keiyasi Action Plan).
Mr Timothy Young closed the meeting by commenting on the prevailing attitude that it was the
Government's responsibility to solve the environmental health problems in the village. He asked
the question "who is the Government?" and pointed out that it is actually people like himself and
the Environmental Health Officers present at the meeting, and that the solutions can only come
from the community itself, with the support and understanding of Government personnel.
A quick evaluation of the Keiyasi Workshop was carried out by asking the participants to provide
feedback on the Workshop. Comments from the Village spokesman and other participants
included the following:
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[15]
Ę The people were not aware that allowing animals loose in the village would create health
problems, as it was the norm to allow pigs and horses in the village.
Ę New knowledge had been brought to the village about decreasing the number of sick people
taken to the hospital by improving hygiene conditions in the village including proper rubbish
disposal and animal management.
Ę The CT is useful to know about and totally new Ł good to know that the system will last for
many years.
Ę Helpful to learn how to develop an Action Plan Ł ongoing support is needed and it would help
if health officials return to see the improvements the village has achieved as a result of what
they have learnt during the Workshop.
Ę The Workshop could have been improved by hands-on training for building CTs in the village,
and in general to provide live/real demonstrations to assist the participants to grasp the
objectives of the Workshop Ł consideration should be given to the "poor educational
background" of the villagers.
Observations made by the Project Team during the Workshop include the following:
Ę Participation and involvement in the Workshop appeared to be assisted by the active
presence of the Chief for the whole event, and the attendance at the Suva training by the
Head Man and his subsequent presentation to the Workshop.
Ę Billeting of the Project Team in the village for three days allowed some relationships to be
developed between Project personnel and the community and this appeared to also assist
with interest and participation.
Ę Participants were more likely to ask detailed questions especially about the CT when the
opportunity for informal contact occurred throughout the meeting e.g. during meal times or
during the small group discussions Ł twelve participants approached the Consultant to
discuss the CT, in English, over the two days.
Ę Keiyasi only had reticulated water for a couple of hours a day, and households had to pay for
their water usage, so a toilet, which did not use water, and did not need to be moved around
(such as is required with a pit latrine) had immediate practical appeal.
Ę News about the CT spread through the village after the first day and additional participants
attended on the second day. As there were no further presentations about the CT on the
second day, information was provided outside the meeting. People were interested in building
the CT at their homes in the Keiyasi District and on their home islands such as the Yasawas.
Saving water seemed to be the main motivation.
Ę Both women and men were actively involved in the Workshop asking questions, making
comments and presenting their Action Plans.
Ę It appeared that the sanitary well, the VIP and the septic with soakage trench required more
emphasis in the Workshop so that people understood that these systems also needed
attention to be properly designed, located, constructed and maintained.
Keiyasi did not seem to have sufficient understanding that any kind of sanitation systems should
be properly constructed and maintained in order to maintain public health and protect the
environment. This includes the essential requirement for septics (and soakage trenches) and pit
latrines to be safely located in relation to water resources and human activities.
Taking this into account, this aspect of the Sanitation Park and any further related training needs
should be strongly emphasised, demonstrated and discussed to ensure understanding.
It should be noted that the same principles of adequate treatment and location applies to
discharge from a reticulated sewerage system.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]

[16]
Balevuto Workshop, 21-22 June 2004
Figure 3:
Ba Environmental
Health officers present
at the Balevuto
Workshop
Representatives from the nearby villages of Toge and Nadrugu joined the Balevuto community
members for the Workshop. The communities grew sugar cane, pine trees and vegetables.
On June 21, the Workshop opened with an isevu sevu followed by an introduction by MoH
officers, Mr Timothy Young and Ms Vasemaca Naulumatua, explaining the Sanitation Park
concept and the Healthy Islands programme. The rate of decomposition of various types of
rubbish was discussed. Some participants commented that the local Ministry of Health clinic was
untidy, so that should be cleaned up first before Environmental Health Officers gave advice about
rubbish in Balevuto. It was pointed out to them that the clinic was part of the community's
responsibility.
Environmental Health Officer, Mr Vitale Varo, presented a profile of the three villages. He had
attended the Sanitation Park training in Suva so he then presented the slides of the CT
construction. The community representative Mr Samisoni Tukana who had attended the training
was reluctant to speak. While he had been actively involved in the CT construction he was unable
to present what he had learnt to his community in the formal context.
There were problems with lighting in the community hall where the Workshop was held so it was
not possible to show the video of Australian CTs as the VCR did not work and the DVD `Water
Tomorrow' was shown but it was very difficult to see.
Questions that followed after the CT presentation included the following:
Ę How can we get funding to have a CT built in the village to try it out? Need to follow the
procedure through the District Officer;
Ę What are some of the problems that can happen with the CT? The system should be kept dry,
and dry leaves have to be collected to use in the toilet; and
Ę What happens if we use water? The system will not compost the waste and it could smell.
The participants then broke into their village groups and prioritised the issues that needed
attention in the village. Water supply and toilets were listed but septic tanks were the desired
option.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[17]
Part of the Project Team stayed back in the community after the Workshop was completed on the
first day resulting in further discussions with other community members. This resulted in the slide
show about the CT construction being shown again at the opening of the second day.
For the remainder of the day, the community representatives prepared the action plans for their
villages. Toilets and water supply were listed as priorities but flush toilets with septic tanks were
the desired system. Ms Naulumatua was unable to attend on the second day so the activities for
developing the Action Plan were coordinated by the local District Health Worker. The action plans
were presented back to the larger group at the end of the Workshop (see Annex E for Balevuto
Action Plan).
There was no formal evaluation of the Workshop by the participants but there generally appeared
to be less participation and interest than was shown at the Keiyasi Workshop.
This could have been influenced by a number of factors such as:
Ę The local Chief did not attend the Workshop.
Ę The community representative at the Sanitation Park training was not a senior member of the
village and it appears he had not informed the village about the training, as most participants
did not know what the Workshop was about.
Ę The Project Team did not stay in the village and so there was little time to make a connection
with the community. The overall relationship did appear to improve on the second day
following several members of the Project Team staying back to socialise in the community the
previous evening.
Ę The male participants drank kava throughout the whole Workshop;
Ę The women remained at the back of the hall and only became involved during the
development of the Action Plan. It appeared that most of the women of Balevuto were
engaged outside preparing the lunch and morning and afternoon tea.
Ę Once again the issues associated with proper use of septic tanks, VIPs and sanitary wells did
not appear to have been absorbed by the participants.
As in the case of Keiyasi, Balevuto also did not seem to have sufficient understanding that any
kind of sanitation systems should be properly constructed and maintained in order to maintain
public health and protect the environment. This includes the essential requirement for septics
(and soakage trenches) and pit latrines to be safely located in relation to water resources and
human activities.
Taking this into account, this aspect of the Sanitation Park and any further related training needs
should be strongly emphasised, demonstrated and discussed to ensure understanding.
It should be noted that the same principles of adequate treatment and location applies to
discharge from a reticulated sewerage system.
Nadelei Workshop, 1-2 July 2004
The final in the series of community Workshops was held in Nadelei on the 1st and 2nd of July
2004. Representatives from the nearby village of Waikubukubu also joined the Nadelei
community members for the Workshop.
On July 1, MoH officers, Mr Timothy Young and Ms Vasemaca Naulumatua explained about the
Sanitation Park and the WHO Healthy Islands Programme; opening the Workshop in a similar
fashion to the two preceding workshops with an isevu sevu followed by an introduction.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]

[18]
The Workshop in Nadelei was different in that there was a stronger FSchM presence than the
previous two workshops with Mr Navi Litidamu, Mr Nemani Seru and three active FSchM students
who had formed strong links with the community while working in the area as part of the FSchM
student programme. The three FSchM students presented the village profile for Nadelei back to
the community. It was seen that FSchM took the lead on facilitating the group work and action
plan development for the Workshop in Nadelei.
Additionally, the community representative Mr Semi Koroi, who had attended the hands-on
training in May was a strong advocate for the programme in the community and had briefed them
already on what he had learned prior to the Workshop, which complemented and supported the
Workshop programme.
Following on from what the FSchM students had presented, Mr Koroi then made a brief
presentation to the Community on the training he received during the CT construction training
using the slide show prepared by the Consultant.
In the case of Nadelei, the community hall was dark enough to allow the screening of the DVD,
"Water Tomorrow" to be effective which allowed the community to see experiences from Tonga
and Kiribati.
For the remainder of the day and the beginning of the second day, the community separated into
their various villages and prepared the Action Plans for their villages accordingly. This was
presented back to the larger group at the end of the Workshop (see Annex F for Nadelei Action
Plan).
Figure 4:
Group discussions and
formulating action plan at
Nadelei Village.
There was no formal evaluation of the Workshop by the participants but general impressions by
the Project Team was that there appeared to be a lot more participation from the community,
similar to what was shown in Keiyasi.
This could have been influenced by a number of factors such as:
Ę The community member involved in the hands-on training exercise was a respected member
in the community and carried the information to them following on from the training which
supported the Workshop programme when carried out later in the community.
Ę The FSchM played a leading role in the development of the action plans and facilitated a lot of
the discussion between community members and community members and the Project Team.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]

[19]
Ę The venue and environment in which the Workshop was carried out supported the smooth
running of the programme, e.g. dark hall for DVD, direct access to electricity.
Ę Kava was drunk during the isevu sevu ceremony then ceased during the actual Workshop
programme.
Ę Although the women were involved in the preparation and serving of food they had also
organised themselves to also be able to participate in the Workshop programme as well.
Ę The programme was amended somewhat to incorporate issues associated with proper use of
septic tanks, VIPs and sanitary wells, which was not delivered as effectively during the
previous two community workshops.
Sanitation Park Opening Ceremony, 18 November 2004
Figure 5:
Acting New Zealand High
Commissioner, Ms Joanna
Kempkers and Dr Sitaleki
Finau of the Fiji School of
Medicine, at the opening of
the Sanitation Park.
The Sanitation Park Opening Ceremony held on 18 November 2004 was crowning glory event of
the Sanitation Park Project, completing the implementation of all its components.
The Chief Guest for the Opening was Ms Joanna Kempkers, Acting High Commissioner, New
Zealand High Commission, who provided an insight into NZAID Health Policy and links with a
Project like the Sanitation Park for which it partly funded together with WHO.
The Opening Ceremony provided an opportunity to showcase the Park to the general public from
various sectors. Guests provided interesting feedback Ł one mentioned that they never actually
knew nor thought much about what happened after the "waste" disappeared down the toilet,
which was the desired effect.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[20]
4: PROJECT CONCLUSIONS AND RECOMMENDATIONS
From concept to implementation the Sanitation Project took four years to carry out, with funding
being secured at various stages of the Project.
Generally, the strengths brought to the Project Team by the various partners allowed for the
various components to be implemented in an effective manner with each partner providing the
skills needed to deliver on the various components (see Annex G for Project Partners MOU).
The following recommendations and conclusions can be drawn from the various components:
Recommendations from Construction of Sanitation Park
It must be noted that these recommendations are being made in the context of the construction of
the Sanitation Demonstration Park at the Fiji School of Medicine, Tamavua Campus and does not
in any way apply to community experiences.
The construction of the Sanitation Park and the development and installation of signage took one
year to implement. Recommendations by the Project Team for this component of the Project
include the following:
Ę In the Project planning stage, account for more time (at least six months) for construction than
originally planned as experience from the Project has shown that time taken for construction
over-ran the original plan by several months.
Ę Budget in more than planned for, when dealing with construction, as prices often fluctuate
which can significantly affect budgets and often there is more work and materials required
than was originally planned for once construction gets underway and unfolds.
Ę A skilled, innovative and reliable builder is an important quality to deliver on construction of
Projects. We were fortunate to have been able to secure Mr Rakesh Dayal for the Project who
in addition to carrying out work specifically outlined in his TOR, also facilitated training when
called upon during the hands-on training exercise.
Ę Contracting out construction for the building of systems under the supervision of the Project
Team worked out well with the SOPAC purchasing materials from local supplier (GMR) for
builder on request to carry out work at site. From this experience, we recommend the use of a
skilled, innovative and reliable builder be considered for the construction works with the
Project Team purchasing materials for construction when needed.
Ę There is a need to develop a seat or pedestal for use with CTs in Fiji. The seat should be easy
to move when the first chamber is full, and manufacturer to also provide a hygienic seal for
the first chamber when the seat/pedestal is installed above the second chamber.
Ę When dealing with several individuals in a Project Team discussing issues with regards to
signage information, system features and design, it is important to note that this is time
consuming and needs to be accounted for in a Project timeline. Extra time should also be
entertained for this component because final products will be in place for a long time and is
often difficult to change when in place.
Recommendations from the Community Programme
The community programme included the Hands-on Composting Toilet Training at the Sanitation
Park and the subsequent community workshops in Keiyasi, Balevuto and Nadelei. Lessons
learned by the consultant and the Project Team during the community programme are outlined
below:
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[21]
Ę Practical hands-on training is an effective way to promote a sanitation system and convey the
principles behind the approach. People are empowered by learning technical skills and
knowing that they can make well-informed choices, and that they can construct and maintain
the systems themselves.
Ę Where it is necessary to provide additional or background information to trainees it should be
short (not more than 30 minutes) well-illustrated presentations preferably with a human story
line e.g. children using the system or dealing with problems of maintenance etc.
Ę Power Point presentations should be carefully used to enhance the information presented
through the use of photographs and clear relevant diagrams, but not as a substitute for
engaging communication. Using Power Point to present lengthy text or impersonal data can
create a barrier to understanding and interest in any culture.
Ę Where media such as DVDs and video are shown the equipment should be tested in
advance, in the Workshop setting, so that the participants are not left waiting while technical
problems are solved.
Ę Having trainees present what they have learnt to their community is an effective method to
reinforce and clarify the message, but it is also important that the trainee has the confidence
and ability to explain the information in a public setting.
Ę Overall participation and understanding in a community appears to be increased by the active
involvement of women in the practical training, discussion and decision-making. It may be
necessary to ensure that women are not prevented from attending the Workshop because
they are taking care of the catering.
Ę Staying in a village for a number of days and working through the village leadership and
established networks can increase the potential for interest and involvement by the
community.
Ę As every situation is different it is necessary to be prepared for a variety of outcomes in a
Workshop context. Participation and effective communication is influenced by many factors,
including the personalities and status of the facilitators and the participants who are involved,
and their relationship with each other.
The combined recommendations have revealed methods for carrying out similar Projects in the
future. Some of the methodology used in the Project can be repeated and other things could be
done differently depending on the context of the future situations. These recommendations are
not meant to be rigid rules but to be used as guidelines.
Conclusions
The future actions issuing out of the Project will involve communities implementing action plans
developed during the community workshops, which will be managed by the MoH in their
programmes throughout the various districts.
The long-term management of the Sanitation Park has become the responsibility of FSchM,
where the park can be used as a training tool for students and community workers. They will also
develop training material to complement the systems at the Park.
Finally, the Park will be open for visitors from communities, schools and other training institutes
as it is a very good well-presented tool to use when trying to raise greater awareness of available
technologies for wastewater treatment; with its cut-away models and simple signage messages.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]

[22]
ANNEX A: PRE-PROJECT SURVEY INFORMATION APRIL 1ST-30TH APRIL 2000
Viti Levu, Fiji Islands
1. Survey Schedule
The 5-week survey targeted fourteen communities.
Survey Schedule was as follows:
Week 1: Navua 06/04/00
(Nabukelevu settlement): Population 289
Week 2: Sigatoka Ł Nadi 13/04/00
Sigatoka (Malolo Indian Settlement): Population 102
(Keiyasi Village): Population 91
Nadi (Mulomulo Village): Population 138
(Nabila Indian Settlement): Population 222
Week 3: Lautoka, Ba, Tavua, Rakiraki 17-20/04/00
Lautoka (Vunato): Population 132
Ba (Balevuto) Population 191
Tavua (Nadelei Village): Population 315
Rakiraki (Matainubu Settlement): Population 23
(Naseroi): Population 53
Week 4: Tailevu 25/04/00, Suva 27/04/00
Tailevu (Vorovoro): Population 154
Suva (Bureta Settlement)
Week 5: Suva 02/05/00
Matata: Population 230
Nabaka
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[23]
2. Information Gathered from District Health Offices in Checklists
Ę Nabukelevu settlement, Serua Ł situated inland (interior), some (22 km) 2 hrs drive on
gravelled (unsealed) road from the main Suva/Nadi Highway. The main source of income
is from agriculture, where root crops such as dalo, cassava, and yaqona are grown on a
small scale. With a population of over 280 people and 41 households. Cases of diarrhoea,
worm infection and skin infection are common.
Ę Naqelekuga Mataqali, Keiyasi, Sigatoka district, interior, population of 91 with 18
households. 60 km away from main urban centre, Sigatoka, unsealed road. Checklist
showed there were 23 cases of diarrhoea over the past two years.
Ę Malomalo, Sigatoka, with population of 102 and 14 households. 30 km from main urban
centre Sigatoka on unsealed road. Checklist showed water supply is from boreholes.
Reported 12 cases of diarrhoea over the past two years.
Ę Vunato, Vitogo, Lautoka, situated in coastal area, with 132 population and 22 households.
Į km from main urban centre, Lautoka. Mainly piped water supply and poor sanitary
condition. Cases of sanitary diseases, such as diarrhoea 20, dysentery 15, worm infection
(hookworm) 12 and dengue fever 7, over the past two years.
Ę Nadelei, Tavua situated in the interior, population of 315 with 63 households. 14 km from
urban centre, unsealed roads. 18 cases of diarrhoea, most of which are not reported such
as cholera, worm infection and dengue.
Ę Matata, Lami, Suva situated in the interior with 230 people, and 46 households. About 10
km from Suva which is the nearest urban centre on unsealed roads. Cases such as 31
diarrhoea and 20 dysentery were reported in the last two years.
Ę Vorovoro in the Sawakasa District Tailevu. Situated in the interior with 154 people and 29
households, accessible through unsealed roads. Cases of infertile diarrhoea and
dysentery.
3. Pre-Project Survey Team
The Pre-Project Survey Team included, two SOPAC staff, 10 FSchM Students (5 pairs), FSchM
Senior Staff member and 1 Ministry of Health District Officer
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[24]
4. Household Survey Questionnaires
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]

[25]
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[26]
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[27]
lo
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[28]
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[29]
The Survey questionnaire was translated into Fijian and Hindi for use in the communities and was
used by the Project Team together with the community members.
General Observations of the Survey Team:
Ę Not all questions answered properly.
Ę Confusion in answering individual multiple questions.
Ę Some questions found to be irrelevant.
Ę Unanswered (blanks).
Ę 14 Villages surveyed only 12 identified as valid.
Ę OMITTED: Rakiraki (Matainubu Settlement): Population 23, and (Naseroi): Population 53 as
there were only two households that had members not at home in these settlements at the
time of survey, as most of the people had left for some event out of town.
Data collected from the survey was entered into a SPSS Data Editor, a qualitative statistical
analysis programme. This programme is designed for inputting data and analysing variables. In
general the survey gave the following results:
At the Household level:
Ę Total of 270 households and 390 individuals interviewed.
Ę 66% of families live in nuclear families.
Ę Majority of the families have four to eight members in the family with over 21% having an
average of six in the family.
Ę Ethnic distribution: About 85% of the survey consisted of Fijians and 15% Indians.
Ę Education: Majority of the population have junior secondary as the highest education level.
(8%) more females have no formal education.
Ę Occupation: 66% depend on agricultural produce as their main source of income.
Ę Water Supply: About 40% of all villages receive their water supply unmetered from the main
PWD water source. Alternatives were metered water supply (30%), well water (22%),
roof/tank catchment (18%), river/creek (20%), communal standpipe (10%).
Ę Only 12% indicated their water supply quality as poor.
Ę 32% indicated that water dries up every year, and 40% said occasionally.
Ę Problems with water supply: 44% complained of low pressure, 30% reported leaky pipes.
Ę Type of toilet: 43% use water seal privy, 36% use pit latrines, and only 18% use flush toilet
types.
Ę Social Amenities Score: Over 70% of population live below the 4 score.
At individual Household Member level:
Ę 50% wash hands with soap, 48% with just water and 2% do not wash hands.
Ę 30% boil drinking water, 42% sometimes and 30% do not.
Ę 11% do not know what diarrhoea is.
Ę 14% said they had diarrhoea in the last two weeks.
Ę Waste water disposal system: septic tank: 25% had this either private or shared.
Ę 75% indicated that there is no disposal system and often used a simple ground drainage
system since 35% used pit latrines.
Ę In all 12 villages, majority of the workers are in the agricultural sector.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[30]
Ę The highest educated are in tertiary levels but are in very low numbers. The average level of
education is junior secondary for both males and females. Nadelei showed the most number
of educated people. There are more educated males in tertiary level overall.
Ę Three villages considered sanitation a priority, Keiyasi, Balevuto and Nadelei.
A review of the questionnaire results showed Keiyasi, Balevuto and Nadelei considering
sanitation as a priority and was a determining factor in choosing these communities for the
Project.
5. Water Quality
During the survey, water quality tests were also carried out using modest equipment gathered
from members of the Project Team. The intention of the water quality tests was to get an
understanding for the current situation with regards to water quality. Samples were collected from
nearby water bodies such as rivers and also from the drinking sources such as wells, rainwater
tanks, and taps.
General Results of the survey are as follows:
Ę pH levels were found to range from 6.7 to 8 with an average of 6.8. Standard of pH levels are
6.5 to 8.5 thus the levels found are acceptable.
Ę Turbidity: Standard level is 5 NTU, results show levels as high as over 250 to as low as 0
NTU.
Ę Temperature: Averaging 27░C
Ę Salinity: testing also showed low levels of minerals indicating salt content.
Ę Chlorine: No chlorine found in all samples taken.
Ę Nitrite: Standard = 1
Ę Nitrate: Standard = 10
Ę Sulphate: Standard = 250
Ę Faecal Coliform: Nabukelevu Village, outside of Navua showed the highest level of Faecal
Coliform counts. An average of 30% coliform growth was seen in most village water supplies.
The results from the water quality survey cannot be substantiated as samples were taken in the
field using equipment that was outdated and not properly calibrated therefore water quality
information was not used as a basis for making decisions on which communities were chosen for
Project implementation.
6. Geographical Information System
GIS information was gathered by the SOPAC Team for the majority of the communities surveyed,
however there was a technical fault with the equipment which resulted in only three data sets
being processed for only three communities.
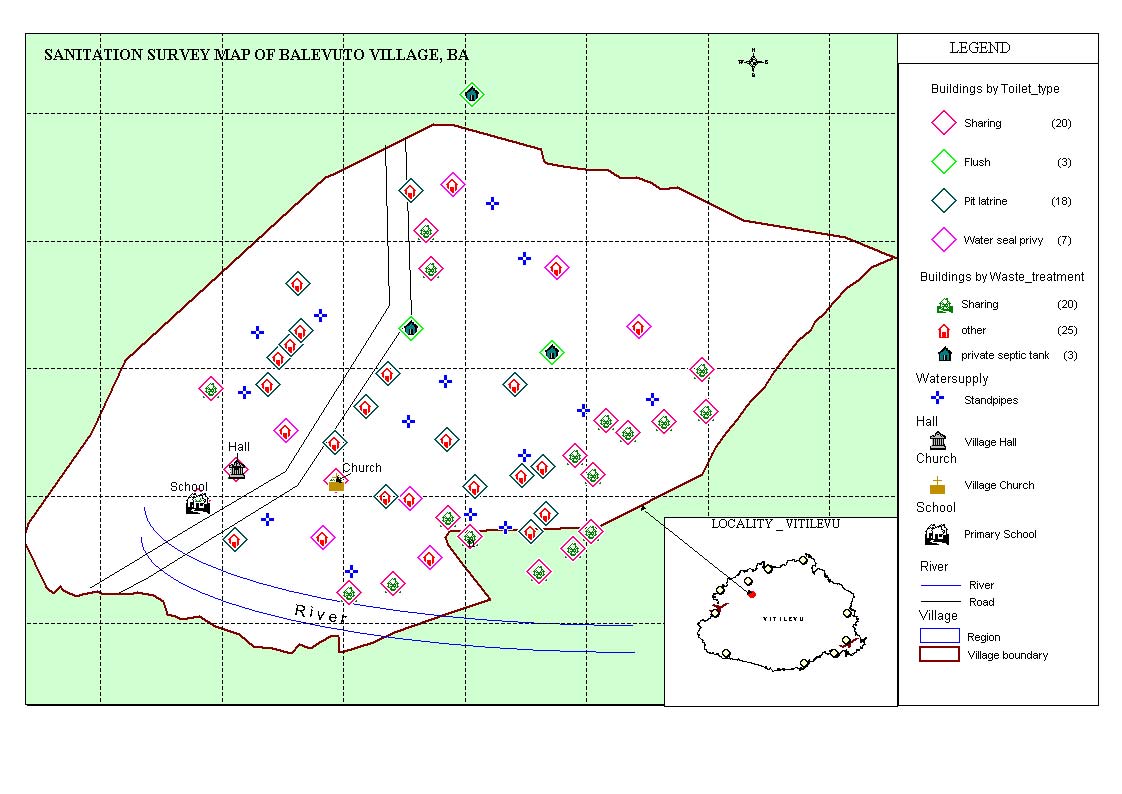
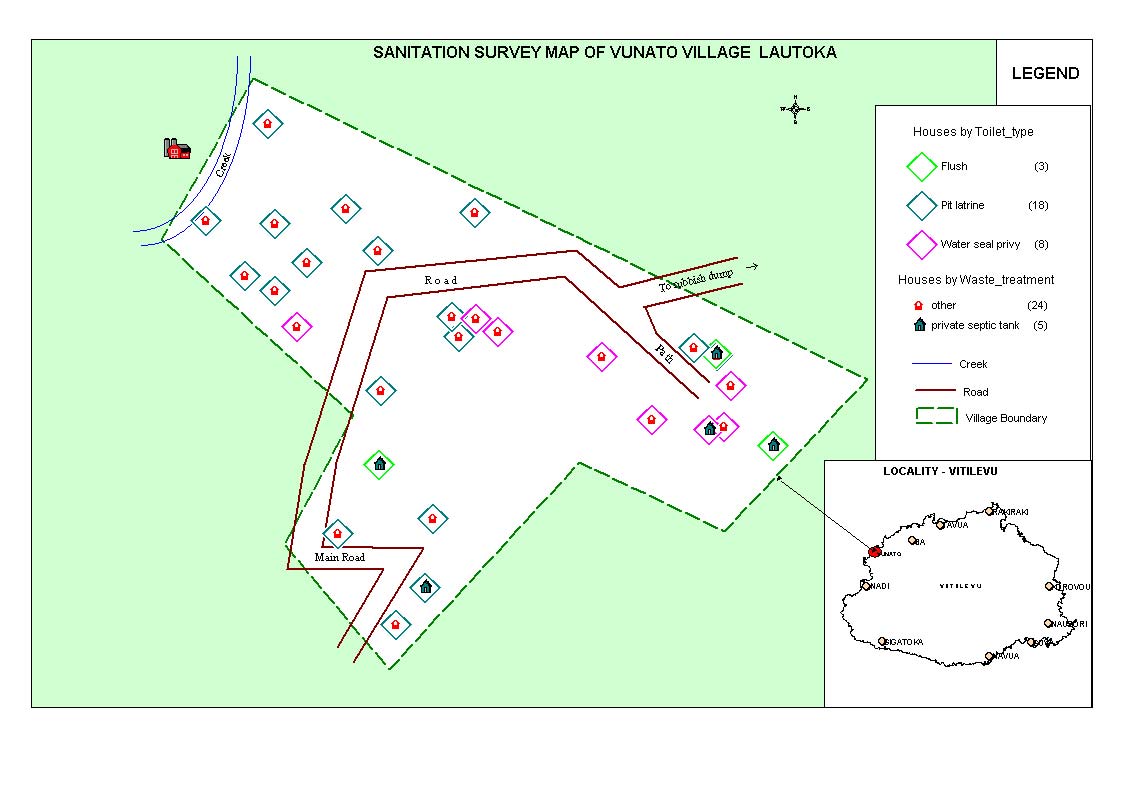
The three villages for which data was successfully captured and processed were (Vunato)
Lautoka, (Balevuto) Ba, and (Nabukelevu) Navua.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[31]
Balevuto, Ba
Map indicates 48 houses,
a church, a school and a
village hall. There are
about 14 communal
standpipes spaced out
around the village
grounds. An average of
three houses to a
standpipe, thus easy
access to water supply.
Water is pumped from
the river direct to the
standpipes. There is no
treatment of water.
The river is also used for
washing clothes, drinking
water for livestock and
bathing.
Vunato, Lautoka
Vunato is more of a
settlement then a village,
located just outside of
Lautoka city; there are
about 30 houses. Each
house has its own piped
metered water supplied
from the Public Works
Department. No
communal standpipes
have been indicated. The
main road passing
through the settlement
leads to the City rubbish
dump. Daily dump trucks
drive through the village.
A narrow creek littered
with debris runs behind a
row of houses.
Across the creek is the industrial area, which emits smoke and discharges waste into the creek. The settlement
area is based on marshy grounds with poor drainage system.
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[32]
ANNEX B: HANDS-ON TRAINING WORKSHOP PARTICIPANTS LIST
MAY 2004
Name Organisation/Address
Contact
Mesake Biumaiwai
Keiyasi Village, Navosa
Penioni Cagilaba
Keiyasi Health Office
Samisoni Tukana
Balevuto Village, Ba
Vitale Varo
Ba Health Office
Tel: 6674045
Sofaia Tatatau
Tavua Health Office
Tel: 668 0500
E-mail: sofaia@connect.com.fj
Semi Koroi
Nadelei Village, Tavua
Niko Nadolo
FSchM student
E-mail:S019093@fsm.ac.fj
Mele Turagavou
FSchM student
E-mail:S019073@fsm.ac.fj
Pritika Edwina Raju
FSchM student
E-mail:S030793@fsm.ac.fj
Mary Ackley
US Peace Corps/Vunisinu
E-mail:ma_pcorps@yahoo.com
Pita Vatucawaqa
Vunisinu Village
Kelera Oli
Fiji School of Medicine
E-mail:S952551@fsm.ac.fj
Naresh Narayan
Fiji School of Medicine
E-mail: S004614@fsm.ac.fj
Rota Takula
FSchM Student
E-mail: S030776@fsm.ac.fj
Timothy Young
Ministry of Health, Suva
Navi Litidamu
Fiji School of Medicine
Keshwa Nand
Tamavua Campus
Suva
Leonie Crennan
SOPAC Secretariat
Leonie@sopac.org
rhonda@sopac.org
Rhonda Bower
Private Mail Bag
arieta@sopac.org
Arieta Navatoga
Suva
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[33]
ANNEX C: COMMUNITY HEALTHY ISLANDS WORKSHOPS PARTICIPANTS LISTS
JUNE 2004
Community Workshop 1 Ł Keiyasi Village, Sigatoka Ł 16th-17th June 2004
NAME
VILLAGE
1.
Nasoni Kuriyago
Keiyasi
2 Ravuama
Kuriloa
Draiba
3 Uraia
Davu
Edrau
4 Vinaya
Waka
Edrau
5 Simione
Gusuivalu
Keiyasi
6 Eroni
Sau
Edrau
7 Viliame
Veto
Sawenw
8 Batiniloka
Nadule
Sawene
9 Waisea
Toutou
Edrau
10 Apisaki
Matawalu
Keiyasi
11 Aseri
Turagadrau
Keiyasi
12
Salome Latilevu
Navula
13 Taraivini
Bula
Keiyasi
14 Lotawa
Naliva
Navula
15 Titilia
Leiroti
Keiyasi
16 Miriama
Kadavu
Nalovosa
17 Anaseini
Bolakoro
Navula
18 Manaini
Ravela
Nalovosa
19 Alivani
Leano
Nalovosa
20 Litiana
Lalilevu
Nalovosa
21 Titilia
Vatiseva
Nalovosa
22 Lereani
Novo
Navula
23 Simione
Loli
Keiyasi
24 Makitalena
Voli
Natao
25 Litia
Navukula
Keiyasi
26 Titilia
Ratudradra
Keiyasi
27 Salaseini
Roko
Draiba
28 Jonasa
Tui
Keiyasi
29 Vara
Nadule
Keiyasi
30 Seruwaia
Baivatu
Keiyasi
31 Aseai
Vialani
Keiyasi
32 Miriama
Kurinacoba
Nalovosa
33 Mereoni
Limaiwale
Keiyasi
34
Seva Matawalu
Keiyasi
35
Ratu Viliame Naliva
Keiyasi
36 Talatala
Cagi
Keiyasi
37 Sainiana
Matanisiga
Keiyasi
38 Vilisi
Naseka
Keiyasi
39 Keleni
Devo
Keiyasi
40 Alini
Cagi
Keiyasi
41 Sainiana
Naivalucava
Keiyasi
42
Ratu Meli Nakasavu
Keiyasi
43 Saimoni
Tiqara
Keiyasi
44 Mesake
Biumaiwai
Keiyasi
Ministy of Health, Sigatoka
1. Penioni Cagilaba
2. Luisa Matararaba
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[34]
Community Workshop 2 : Balevuto Village, Ba, 21st-22nd June 2004
NAME
VILLAGE
1. Neumi
Tabuyaqona
Balevuto
2.
Petero Kubu
Balevuto
3. Marika
Naura
Balevuto
4. Jotame
Vesi
Balevuto
5 Vosaboto
Nadrugu
6. Peni
Naulu
Toge
7 Paula
Tora
Toge
8 Iosefo
Matakobulu
Nadrugu
9 Semi
Kunatani
Balevuto
10 Kaliova
Rasaku
Balevuto
11 Avisake
Tora
Balevuto
12 Veniana
Nadibi
Nadrugu
13
N Botitu
Balevuto
14 Isireli
Nounou
Balevuto
15 Anasa
Valu
Nadrugu
16 Siteri
Masiquna
Balevuto
17
Luke Nabaro
Balevuto
18 Siteri
Senitirau
Balevuto
19 Rota
Vakaloloma
Balevuto
20 Navolioni
Tureau
Balevuto
21 Eparama
Koroi
Balevuto
22 Inoke
Qoro
Balevuto
23 Viliame
Nawau
Balevuto
24 Joseva
Gakobau
Balevuto
25 Tevita
Lewanacu
Balevuto
26 Atama
Rokobati
Balevuto
27 Suliano
Bogileka
Balevuto
28 Joseva
Rasaku
Nadrugu
29 Watisoni
Malua
Balevuto
30 Etuwate
Tabua
Balevuto
31 Lanieta
Tora
Balevuto
32 Jone
Kale
Balevuto
33 Inoke
Rauga
Balevuto
34 Samisoni
Tukana
Balevuto
35
Ratu Sela Lewasau
Balevuto
36
Mareta Vunisa
Balevuto
37 Eroni
Maqala
Balevuto
38 Watisoni
Malua
Balevuto
39
Luke Nabaro II
Balevuto
40 Misikini
Manasa
Balevuto
41 Vilitati
Kina
Balevuto
42 Sitivenusi
Bari
Balevuto
43 Joseva
Ratuba
Balevuto
44 Rupeni
Vutoni
Balevuto
45 Sitiveni
Nasigata
Balevuto
46 Iosevo
Masiquna
Balevuto
47 Ropate
Naigada
Balevuto
48
Rev. Vijay Chandra
Chairman of BRLA
Ministy of Health, BA
1. Vitale Varo
2. Isireli Vuanivono
3. Ifereimi Kubukawa
4. Rosita Mala
5. Ashneet Bhagat
6. Ivona Tavuki
7. Mereseni Narikalea
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[35]
Community Workshop 3: Nadelei Village, Tavua, 30th June Ł 1st July 2004
NAME
VILLAGE
1 Semi
Koroi
Nadelei
2 Susana
Naica
Waikubukubu
3 Naiyaba
Waqawai
Waikubukubu
4 Ilai
Manoa
Nadelei
5 Karolina
Nai
Nadelei
6 Nanise
Ranadi
Nadelei
7 Akanisi
Tabua
Nadelei
8 Vinaisi
Voreqe
Nadelei
9 Sera
Cawai
Nadelei
10 Veniana
Vauvau
Nadelei
11 Suluweti
Nai
Waikubukubu
12 Elena
Fulori
Waikubukubu
13 Miliakere
Nailolo
Nadelei
14 Aliti
Laite
Nadelei
15 Masilina
Ranadi
Nadelei
16 Asinate
Kavetani
Nadelei
17 Alefina
Loli
Nadelei
18 Petero
Loli
Nadelei
19 Sailosi
Vunikuta
Waikubukubu
20 Kaliova
V
Nadelei
21 Meli
Ratu
Waikubukubu
22 Anaseini
Navuni
Waikubukubu
23 Miliakere
Naisola
Waikubukubu
24 Sisilia
Nagone
Nadelei
25 Epeneri
Moceidreke
Nadelei
26 Merewalesi
Natabu
Nadelei
27 Naica
Toutou
Nadelei
28 Merelisoni
Savewa
Nadelei
29 Arieta
Nadumu
Nadelei
30 Degei
Naduruka
Waikubukubu
31 Jovesa
Natoria
Nadelei
32 Luke
Vauvau
Waikubukubu
33 Emosi
Ratuwaqe
Waikubukubu
34 Epeli
Takolevu
Nadelei
35
Paula Nagone 3
Nadelei
36 Tomasi
Ratukavida
Nadelei
37 Jone
Saitabu
Nadelei
38 Sereima
Dela
Nadelei
39 Mere
Lauwai
Nadelei
40 Siteri
Naisu
Nadelei
41 Udite
Nadumu
Nadelei
42 Lavenia
Nasalasala
Nadelei
Ministry of Health, Tavua
1. Sr. M Q Nayasi
2. Staff Aliti Kanata
3.Ifereimi
4. Tarai Nakoli
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[36]
ANNEX D: KEIYASI ACTION PLAN
RESULTS
PROBLEM POLICY
(LAW) STRATEGY TIME-FRAME PERSON
(INIDICATORS)
RESPONSIBLE
Stop animals
Animal policy
Fundraising
July Ł 2004
Village Health
Clean village &
from entering
Committee
surrounding
the village
Three-month plan
Ł October 2004
Village Headman
Fewer people
getting ill
Healthy/rich
vegetation
All
Each house to Fundraising
December 2004
District Officer
ŁHygiene level
1. HEALTH PUBLIC POLICY
households
have own toilet
increase
with own
Request for
Three-yrs plan
Village Health
utilities
government
Committee
ŁVisitors are
assistance
December 2006
happy & satisfied
Village Headman
while staying in
the village
Electricity in All households to
ŁCollect fund
Two-year plan
Village committee
ŁLight in the
the village
have access to
village
electricity power
ŁRequest for
November 2004
Clans headman
government
ŁChildren able to
assistance
November 2006
Village headman &
study at night
through District
District Officer
Officer
To have 24 Each household Fundraising
October 2004 Ł
Village Headman
No problems in
hours supply to have own
having flush toilet
of water in the source of water
Government
August 2004
Village committee
village
assistance
People won't be
2. PHYSICAL ENVIRONMENT
fetching water
from nearby river
for home use
Increase
Support children's Provide support Long term
Parents
Successful
children's
education
& assistance in
education
school
Committee
Decreased
level
unemployment
School Manager
rate for youth
3. SOCIAL ENVIRONMENT
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[37]
Meet all
To help widows, Visit & help
As soon as Women's Club
Happy & healthy
health
elders, sick
regularly
possible
community
problems
Men's Club
especially to
ŁSocial welfare
needy
SERVICES
4. ACCESS TO GOVT. & NON-GOVT.
Increase level Allow education
Request for
Long term
Health Committee
Improvement in
of education
officials to visit
assistance from:
village standard of
and
village regularly
Education
living
knowledge
ŁMinistry of
Committee
Education
ŁMinistry of
Health
Social Committee
ŁPolice Force
5. KNOWLEDGE & SKIILLS
Peace &
Enforce
Sharing
Immediately All
harmony in
socialization
knowledge and
the village or
helping one
Clan headman
any
another
community
Village headman
Church elders
6. COMMUNITY RELATIONS
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[38]
ANNEX E: BALEVUTO ACTION PLAN
PROBLEM POLICY
(LAW)
STRATEGY TIME-FRAME PERSON
RESULTS
RESPONSIBLE
(INIDICATORS)
Existing committee Draw out work
Ł Have regular
Ł Once a week
Village Health
Projects
not productive
plan for each
meetings
Ł Once a month Committee
Funds collected
month and year
Documentation &
Health Department
action
Village headman
Clan headman
Chief
1. HEALTH PUBLIC POLICY
Villagers (all
community members)
1.Water problem
Ł Install bigger
Work together
Every three
Village headman
Install water tank
water tank or
Help each other
months
Village committee
All houses with
Ł Build reservoir Fund raise
Health committee
running tap water
All villagers
Health Department
Regional Office
2. PHYSICAL
ENVIRONMENT
2. Toilet
3.Rubbish disposal
4 Stray animals
Unwanted
Ministry of Health Obey village rules Every three
Heath Dept
No Drug abuse
pregnancy
to conduct
& laws
months
courses at the
Health committee
Drug Abuse
village
Strengthen
Visit once a week
traditional
Village headman
Excessive yaqona Increase people's customs/norms
3. SOCIAL
ENVIRONMENT
consumption
knowledge on
Villagers
health issues
1.No dispensary
Build village
Fundraising
Three months
Health committee
Village nurse
dispensary
Village nurse
present
Seek advice from
Village headman
Drugs needed
Ministry of Health
Village committee
SERVICES 2.Health problems Conduct health
(diseases)
awareness
4. ACCESS TO GOVT &
NON-GOVERNMENT
training
1.School dropouts Community work Workshops
Once a month
Health Dept
Community
2.Unemployment
Support from
Seminars
Village Headman
Awareness on
parents
Health Visit
Villagers
Health Problems
& SKILLS
5. KNOWLEDGE
Weak spiritual
Prayer Meeting
Visit by church
Daily
Reverend
upbringing
elders
Weekly
Preachers
Parents
Village headman
RELATIONS
Villagers
6. COMMUNITY
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[39]
ANNEX F: NADELEI ACTION PLAN
PROBLEM POLICY
(LAW) STRATEGY TIME-FRAME PERSON
RESULTS
RESPONSIBLE
(INIDICATORS)
1. Stray animals
Fence village
Look after own
Village headman' s
All
Ł Lesser no. of sick
animals
day
people
ŁLittering in
Burn, bury or
Daily task
Head of
Ł Healthy clean
river/streams
Properly dispose
decompose
ŁTo begin in August households
surrounding
Łno proper
rubbish
appropriate
Ł Happy family
rubbish dump
rubbish
ŁNo mosquito/
ŁPoor drainage
ŁVillage to have
diseases
proper drain
Ł Construct
ŁPoor toilet
cement drain
ŁOne toilet to each
condition
ŁEach family to
ŁHealth
family
have own toilet
All families to
department
1. HEALTH PUBLIC POLICY
No visit from
facility
build toilets
ŁVillage nurse
Health Officials
ŁVillage health
Frequent visits from
Have monthly visit Village elders to
committee
health officials
make frequent
contacts with
health people
Kitchen Tap
Each family
Timber, roofing
As soon as possible Family members
Clean household
should have one
iron etc
No Village fence
Every Tuesday
Villagers
Clean village
Repair
No proper pig sty
Village meeting
Clean river/streams
To make
Barbed wire
every month
Do not allow pig
sty inside village
fence
2. PHYSICAL ENVIRONMENT
No respect for
Communal work & To possess
As soon as possible Planned by
Peaceful, happy,
one another
gathering
building material
clan/tribe.
healthy village
& equipment
No reconciliation
Prayer meeting
All
Contribute or
Committee
No acceptance by Meeting to be
take part in
members
villagers
held regularly
community work
(once a week)
Disunity in the
Get advice from
village
department of
health &
No government
agriculture
Everyone
assistance
3. SOCIAL ENVIRONMENT
Yaqona to be
Excessive yaqona drunk only on
consumption
special
occasions/appropr
Increased
iate time
adultery
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[40]
No support to the
Invite President of Write a letter to
Last week of every
All
Increase knowledge &
women's club
Fiji Women's
request for:
month
skills
Group
Ł Training by
No visit by govt
govt official on
officials like
handicrafts/sewi
Visit at least once a
All & Government Vibrant, intelligent
health, police and Request for
ng etc
year
departments
skilled youth
as a result
government
concern
problems like drug assistance from
ŁVisit by govt
use, unwanted
officials concern
officials
ACCESS TO GOVT. & NON-
GOVERNMENT SERVICES
pregnancy,
4.
increase school
Hold regular
Organise
dropouts
prayer meeting
awareness day
No support for
All children to
Education
Parents & children Educated children
children in school
attend school
awareness
meetings with
Village committee Decrease
No preschool or
Construct village
children
unemployment
kindergarten
kindergarten
Fund raise
As soon as possible
No school dropouts
5. KNOWLEDGE & SKILLS
No unity
All to be
Elders to be
Have regular
All Successful
responsible in
leading by
meetings &
community
looking after
example
discussion about
welfare of the
problems & how to
village
address them
RELATIONS
6. COMMUNITY
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]

[41]
ANNEX G: MOU PROJECT PARTNERS
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[42]
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]

[43]
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[44]
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[45]
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[46]
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]
[47]
ANNEX H: LIST OF ACRONYMS AND ABBREVIATIONS
CT
Composting
Toilet
FSchM
Fiji School of Medicine
HI
Healthy
Island
HPC
Health Promoting Communities
HQ
Head
Quarters
MoH
Ministry of Health, Fiji
NZAID
New Zealand Agency for International Development
SOPAC
South Pacific Applied Geoscience Commission
VIP
Ventilated Improved Pit
WHO
World Health Organisation
[SOPAC Technical Report 386 Ł Bower, Crennan & Navatoga]